News, Alerts & Events








Optical Plan Information
Please find information relating to the Optical Benefits covered under the Buffalo Teachers Federation Supplemental Benefit Fund below. If you have any questions, please contact the Supplemental Benefit Fund Office at (716) 881-5462.
WHO IS COVERED?
Under the provisions of the BTF supplemental benefit fund optical plan all members, their spouses and dependents under the age of 23 are covered.
WHAT ARE THE BENEFITS?
Covered vision services consist of the care and treatment when performed or prescribed by a physician or a duly licensed optometrist acting within the scope of the license and includes the following:
EYE EXAMINATION
A comprehensive medical examination rendered by a duly licensed physician or a complete vision survey and analysis performed by a duly licensed optometrist.
Teacher Members: $ 45.00 for one examination in a two (2) year period.
Dependents: $ 30.00 for one examination in a two (2) year period.
LENSES AND FRAMES
You are now eligible for a first and second service on both Frames and Lenses (which includes contact lenses) in a two (2)-year period. This means that if you are eligible for a first service and purchase just frames, you are still eligible for a first service on lenses (or vice versa).
A two year period begins on the date of your first service (which is the date you order your glasses) and ends two years later. The next two-year period begins when you apply for benefits after the previous two year period has expired.
If you have any doubts concerning your eligibility, call before you purchase your glasses.
WHAT IS THE REIMBUREMENT PROCESS?
You are responsible for 100 % payment to the optician. After full payment has been made to the optician, mail the completed claim form to the BTF-SBF office for reimbursement.
Claims submitted for reimbursement must be made within six (6) months of the date of service.
Reimbursement may not be paid for any of the following:
Optical Extended Benefits
Please find information relating to the Optical Extended Benefits for Cataract, Glaucoma and Diabetes patients below. If you have any questions, please contact the SBF Office at (716) 881-5462.
PRE‐SURGICAL Cataract Patients
- One (1) eye exam every calendar year
POST‐SURGICAL Cataract Patients
Teachers and their dependents that have been diagnosed as having cataracts and have had surgery to correct them will begin, from the date the surgery takes place, a new two year reimbursement period, regardless of past optical benefit use.
- Four (4) pairs of contacts at the SBF 1st service reimbursement rate (currently $95)
- Four (4) pairs of lenses based on the SBF 1st service reimbursement schedule;
- Two (2) pairs of frames based on the SBF 1st service reimbursement schedule (currently $70).
- One (1) eye examination per year within the new two-year period (currently $50).
At the conclusion of the two-year period, normal benefits would resume.
After the condition has been verified, teachers and their dependents will be eligible every calendar year for:
- Two (2) Glaucoma pressure tests*
- One (1) Visual field test*
Glaucoma sufferers will also be eligible for their normal eye exam once every two (2) years.
* SBF will reimburse each test at the SBF 1st service rate of an Eye Exam (currently $50)
After the condition has been verified, teachers and their dependents will be eligible every calendar year for:
- One (1) eye examination every calendar year
Updated 6/27/18
Optical Payment Schedule
Below find the rates of reimbursement for both eligible teacher members and their spouse and dependent children. If you have any questions, please contact the Supplement Benefit Fund Office at (716) 881-5462.
| Eye Examination | Teacher Member | Spouse & Dependents | ||
| $50.00 | $35.00 | |||
| 1st & 2nd Service | 1st & 2nd Service | |||
| Frames | $70.00 | $60.00 | ||
| Single Vision Lenses | $50.00 | $40.00 | ||
| Bifocal Lenses | $55.00 | $40.00 | ||
| Trifocal Lenses | $75.00 | $55.00 | ||
| Progressive Lenses | $95.00 | $70.00 | ||
| High Index/Polycarbonate | $50.00 | $35.00 | ||
| UV400 |
$18.00 | $15.00 | ||
| Anti-Reflective Coating | $28.00 | $23.00 | ||
| Transition Lenses | $28.00 | $24.00 | ||
| Polarized Lenses |
$23.00 | $19.00 | ||
| Prism Lenses | $6.00 | $6.00 | ||
| Blue Light Lenses | $23.00 |
$20.00 |
||
| Contact Lenses | $95.00 | $60.00 |
THE RATES ABOVE ARE EFFECTIVE ON ALL SERVICES PREFORMED ON OR AFTER JANUARY 1, 2025
Optical Claim Form
The Supplemental Benefit Fund (SBF) does not participate and will not make payment to anyone except the member of the BTF. Therefore, the member is responsible for 100% payment to the optician. After full payment has been made to the optician, mail the completed claim form to the BTF-SBF office for reimbursement. If you have any questions, please contact the SBF at (716) 881-5462.
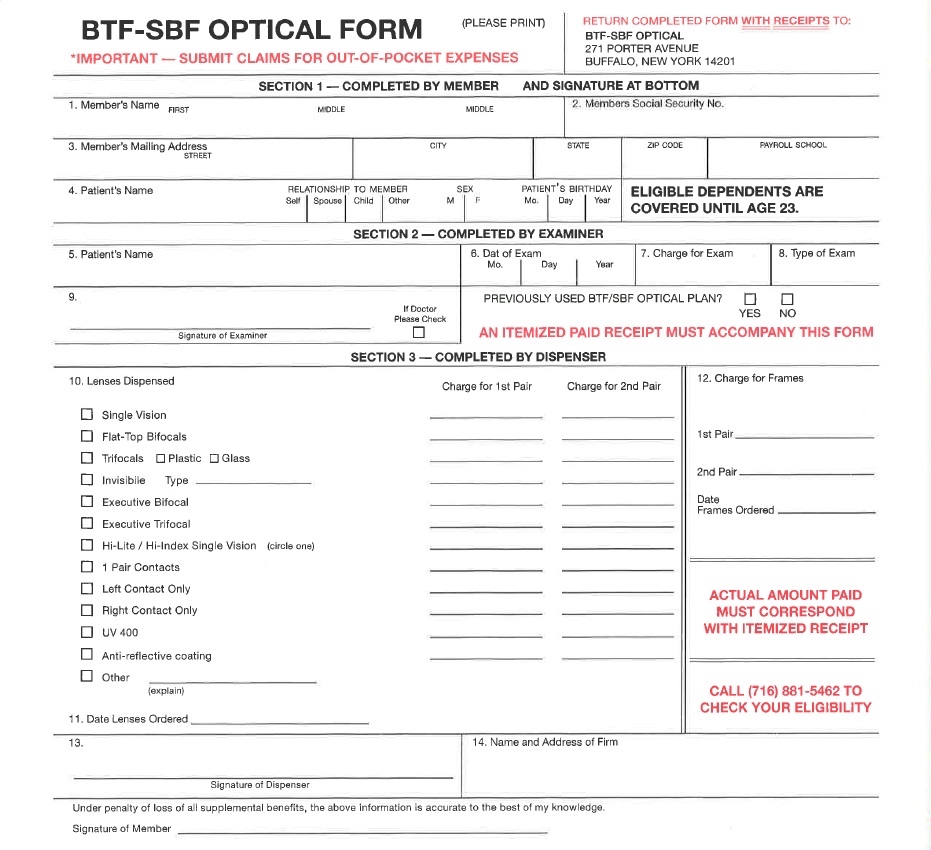
Click on the Image Above to Open and Print the Supplemental Benefit Fund Optical Claim Form
For more information regarding the SBF Optical Benefits, please see the Optical Plan Information Section.
Important Information
Buffalo Teachers Federation

The BTF is proud to be a member of New York State United Teachers and affiliated nationally with the National Education Association and American Federation of Teachers.
We invite you to explore our website for information and resources specifically for our members and retirees.
Calendar
| 13 | Executive Committee Meeting - 5:30 pm | |
| 13 | Council of Delegates Meeting - 7:00 pm | |
| 25 | BTF Retirement Seminar |
| 11 | BTF Office Closed at 4:00 pm | |
| 14-21 | Spring Recess | |
| 24 | Executive Committee Meeting - 5:30 pm | |
| 24 | Council of Delegates Meeting - 7:00 pm | |
Office Information
Buffalo, New York 14201
Fax: 716-881-0580
Guests Online
We have 46 guests and no members online
Did your home address, email address or phone number change? Please let us know! Update Here